


The COVID-19 pandemic, which took the world by surprise at the turn of the year in 2019, brought about two years of insecurity to societies.
Humanity, without immunity against the virus, found itself vulnerable to the unknown disease. With no precise understanding of how the disease was transmitted and how the virus attacked the human body, and with the absence of effective treatment or vaccines, medicine alone was unable to protect everyone.
In this atmosphere of insecurity, mitigation measures and interventions in the built environment had to be devised. These actions had an immediate effect on the daily lives of populations, impacted social customs, and gave rise to new needs and demands.
The COVID-19 health crisis brought several challenges to Architecture, including protecting human life through spatial modifications to prevent the spread of the virus, aiding in maintaining economic continuity through specific changes in commercial spaces, transforming the domestic space into the main stage of daily life, and accelerating the virtualization of work in numerous activities.

Pandemics, mitigation measures, and the consequences of the disaster affect multiple scales, ranging from the global scale to the interior/domestic scale. Understanding the extent of the impacts assists in formulating strategies.
If response actions are not coordinated across all scales, efforts to mitigate the spread of the disease and its consequences are in vain.
The scales of resilience are classified as Mega, Macro, Meso, Micro, and Nano (Figure 1).
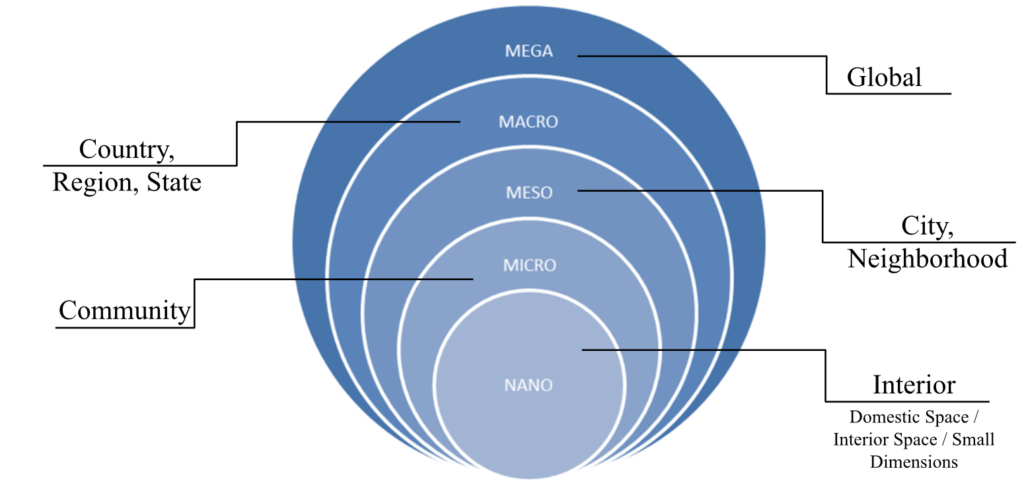
Urban resilience studies that address disaster risks often divide the event into coping phases to define more precise action strategies. In disasters caused by common natural hazards such as floods and hurricanes, coping phases are well-studied and defined. Differently, pandemics are phenomena with a significant short-term impact, resulting in numerous infections and deaths, with consequences that extend over a long period, spanning months and even years. In pandemics, the pre-event phase is well-defined, but the shock does not occur in the same way as natural events. When a new disease emerges, it first starts with an outbreak in a community or neighborhood (microscale), and if not identified and controlled in time, it quickly escalates into an epidemic (meso and macro-scale). Epidemics, particularly in cities with extensive international connections and high transmissibility rates (Rt), have the potential to become a pandemic (mega-scale).
In the case of the COVID-19 pandemic, the initial shock occurred in December 2019 with the detection of the outbreak in the Wuhan market in China. However, the global impact, the major shock, was only realized in March 2020 when the WHO declared it a pandemic.
During the shock and understanding stages, interventions are focused on addressing the immediate needs directly related to the disease. These stages are characterized by saturation of the healthcare and funeral systems, leading to high demand for health and sanitation infrastructure. Advancements in medical sciences allowed the causative agent of COVID-19 to be identified days after the initial outbreak, and its genetic sequence to be mapped eleven days after China alerted the WHO about the emergence of the disease.
Never in history has a new disease been identified so rapidly.
However, it still took several months to understand the transmission mechanisms and the virus’s actions in the human body. The response phase corresponds to the stage where the first spatial and process adaptations are observed in an attempt to mitigate contagion and the pandemic’s effects on all dimensions of the urban system. This phase is marked by strict mitigation measures imposed. Spatial interventions during this stage focus on responding directly to the needs arising from the imposed measures, attempting to adapt spaces to new sanitary requirements. The subsequent phase, recovery, is characterized by the advancement of vaccination efforts and the easing of some restrictive measures, particularly lockdowns. Interventions during this phase are more focused on adapting community and public spaces for reopening. The improvement phase is a period of reflection and assimilation of what has been learned in the previous stages. It typically begins when the disease disappears or becomes endemic. The strategies and interventions reviewed and implemented during this phase are of utmost importance in making the urban system more resilient against future similar phenomena. The last phase is the post-pandemic stage when the urban system returns to its full operational level. However, after experiencing the magnitude of the COVID-19 shock, the urban system may not return to the same pre-pandemic state. After undergoing various adaptations across all system dimensions and going through a prolonged period of learning, the system evolves and reorganizes to a more desirable and resilient state. This approach is directly related to the socio-ecological perception of urban resilience, which views the urban system as a dynamic entity that undergoes transformations after a disruptive event. During the response and recovery stages, a process of self-organization and learning occurs, influencing the system’s equilibrium state (Figure 1). The system may not return to the pre-disaster equilibrium state. Instead, it can recover to a more desired and efficient state than before.





